Happy Twenty twenty too?
In many ways the 2nd year of the COVID19 pandemic was supposed to be better – we had vaccines, new antiviral drugs in the pipeline, monoclonal antibodies and it felt like things would finally get back to normal. The arrival of Omicron in late November 2021 dealt a big blow to these hopes sweeping across the world with lightning speed, leaving chaos and uncertainty in its wake. The new variant of concern (VOC) first identified by scientists in Botswana and South Africa has seen some European countries reinstate lockdown measures, and the United States grapple with upscaling access to rapid diagnostic testing and increasing vaccine uptake.
At the start of this new year 2022, things feel a bit depressing. We all seem resigned to being the next person with a sore throat and that tell-tale dry cough anxiously watching the double lines to appear on a rapid test. Would this year be better? Will we finally learn the lessons the virus has desperately tried to teach us these past two years?

It didn’t have to be this way. From the beginning of the pandemic the threat of new variants of SARSCoV2 had always loomed. This justified the urgency to share vaccines and other resources globally to stay ahead of the virus. “No one is safe until everyone is safe” became the mantra of global health equity advocates everywhere but ignored by those who had the power to do something about it. The legacy of the what was supposed the year of celebrating scientific innovations to end a global pandemic is one of stark division pitting the wealthiest against the most vulnerable.
Promises Not Kept – Vaccine Equity

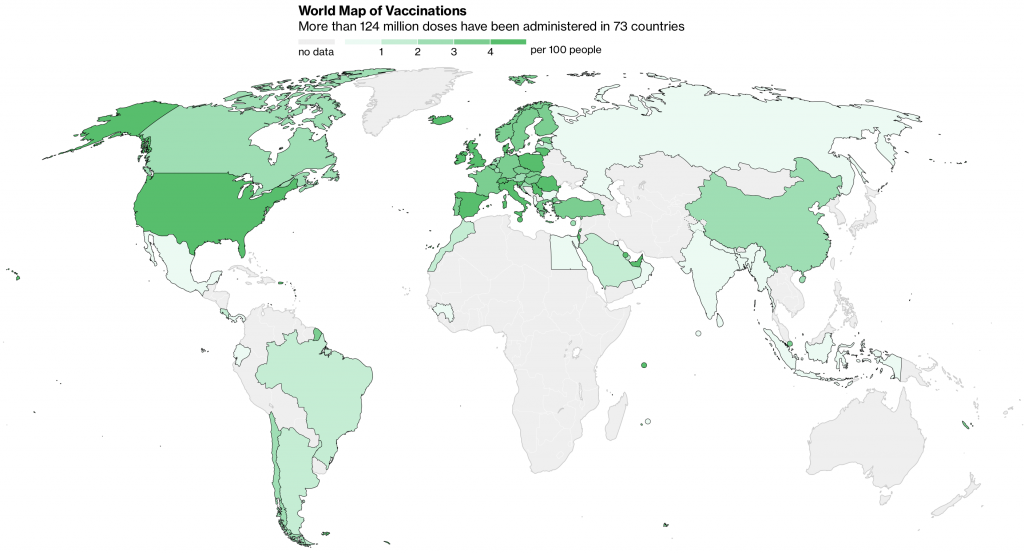
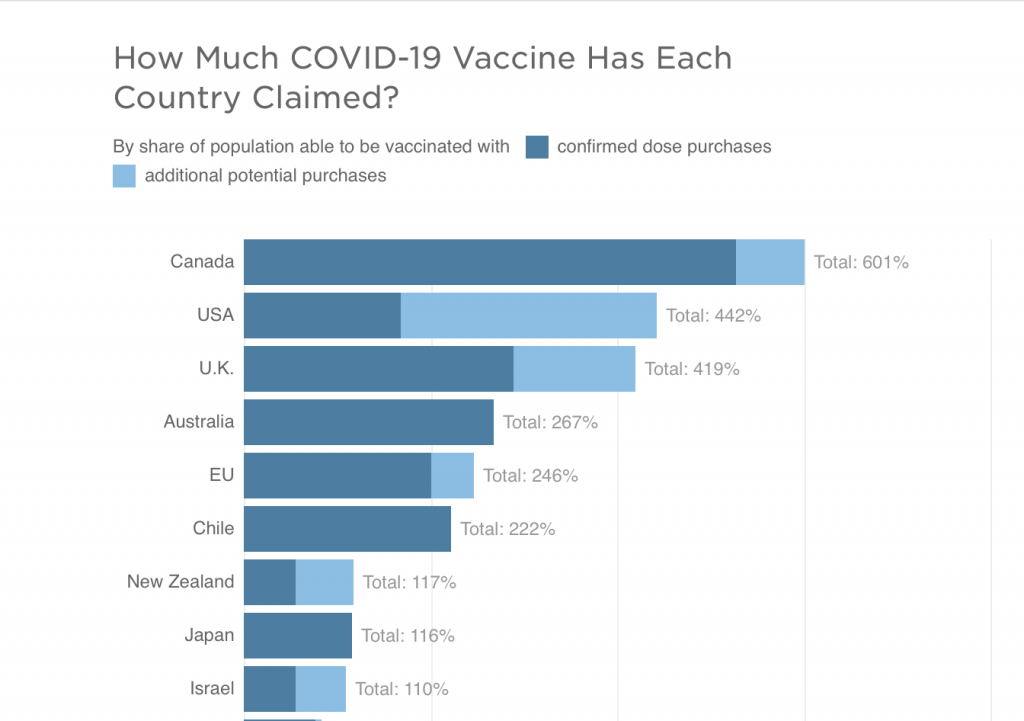
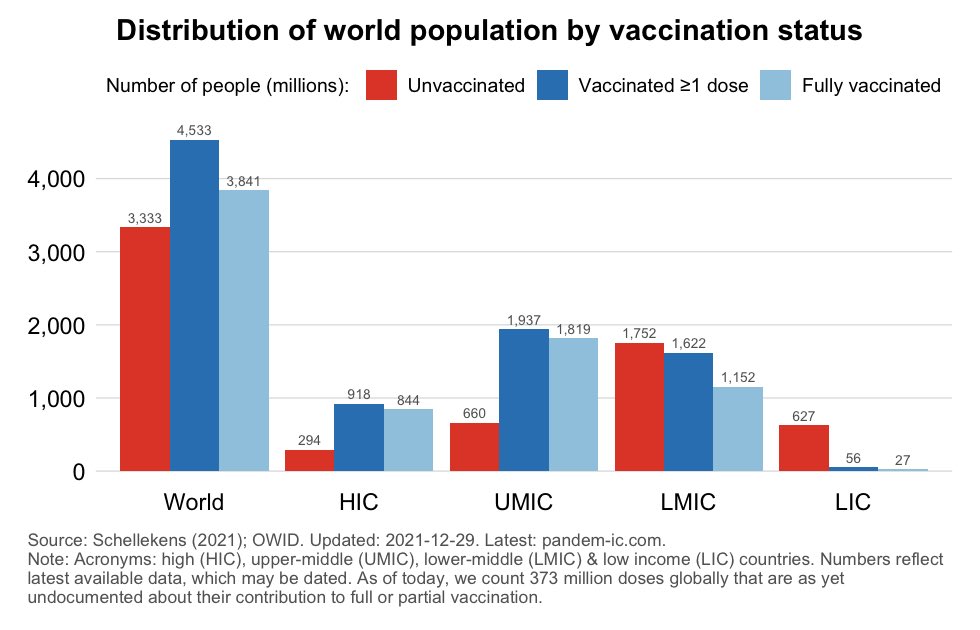
There are 28 vaccines against SARSCoV2 authorized and in use globally. 3.77 billion people have received at least two doses of vaccine. A veritable feat considering that the first vaccines were authorized barely 12 months ago. The rollout of vaccines has been plagued by waning effectiveness against infection, emergence of immune escape variants of the virus, vaccine hesitancy and the failure to deliver on the promise of vaccinating the world. 3.3 billion people mostly in low-income countries are yet to receive a first dose of any vaccine. The main driver of global vaccine inequity the has been the hoarding of available vaccine doses by rich countries purchasing more than needed for their populations. The prospect of intellectual property waivers to ease technology transfer and increase vaccine production in (LMIC) has faded. Key players like Germany have opposed the strategy and stifled negotiations.
All of these factors have been compounded by the need for vaccine booster doses which have increased the pressures on supply and further widened the vaccine accessibility gap. The future of vaccine equity remains uncertain in 2022. Will we see updated second generation vaccines as the older versions become less protective against new variants? Would updated vaccines be available to everyone or will poor countries be left be to rely on older less-effective vaccines? Can global leaders commit to breaking the damaging cycle of vaccine tiering and hoarding? The answers to these questions are known.
It is clear that repeating the mistakes of 2021 is reckless and unlikely to yield different results. Without expanding the capacity of vaccine production in LMICs, the flow of vaccines will remains skewed towards HICs. Distribution of third vaccine doses in the most vaccinated parts of the world currently exceeds first doses in LMICs. Complacency has set in and the chatter about 1st doses before 3rd doses has died down. This doesn’t make the millions of people yet to get their first shots magically disappear but guarantees the virus continued opportunities to spread.

Innovations Not Shared – Monoclonal antibodies, Immunomodulators and Antivirals
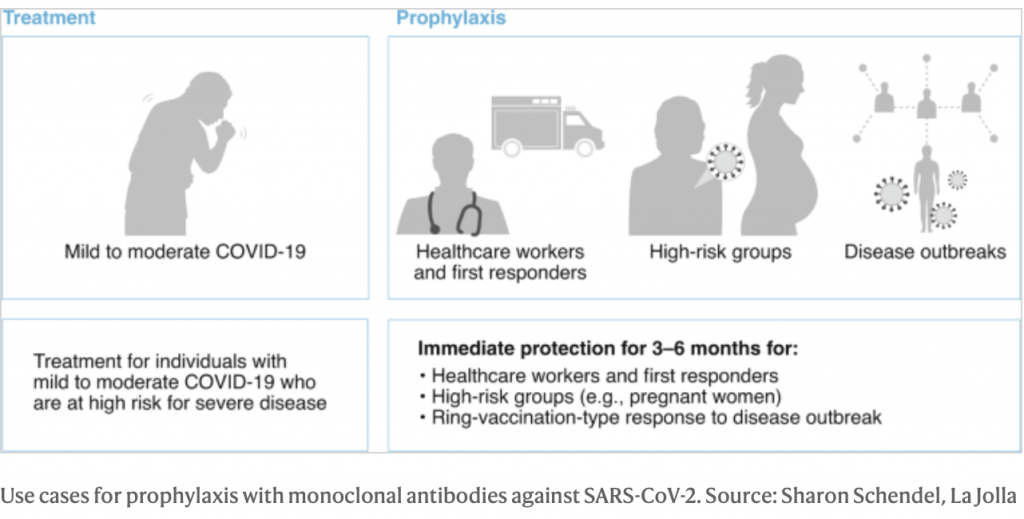
When it comes to therapeutics, we are in a better place starting the new year than 12 months ago. Unfortunately, the scientific progress in the treatment of COVID19 has also been plagued by inequity. Monoclonal antibodies have been a live-saving intervention for millions of people in wealthy countries but beyond reach for poorer countries due to their high cost and the challenges of delivery. Immunomodulatory therapies haven’t fared any better. Dexamethasone is still the sole option in many resource-limited settings despite multiple mortality reducing options.
The end of 2021 brought renewed hope with the authorization of oral antiviral drugs from Pfizer and Merck. High demand and limited supply mean that these drugs may only trickle down to LMICs several months from now. Ideally, countries with fragile health systems, unable to provide a high level of care for severe COVID19 should be prioritized for oral therapies which slow disease progression and keep patients out of hospital. This is unlikely to happen as has been the case with vaccines. Pharmaceutical companies have signed contracts to manufacture lower priced generic versions of these antiviral treatments. However, ramping up supply will take time and limited doses have been secured through advance purchase contracts by high income countries.

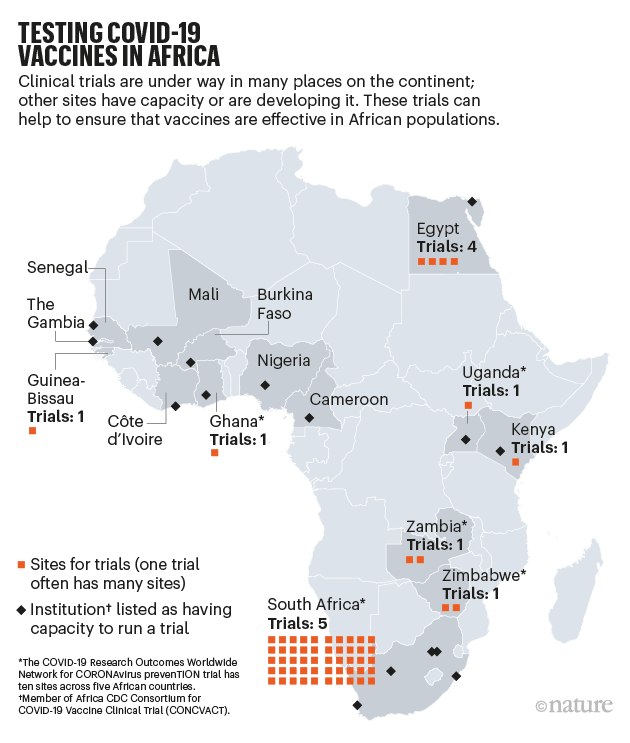
Africa’s Third Pandemic Year
Africa bears the biggest burden of the inequity in accessing vaccines and therapeutic resources for COVID19. Only 9% of the continent’s population is vaccinated. This falls short of the 40% goal set by the WHO at the beginning of 2021. Limited health infrastructure, unsteady vaccine supply, transportation and storage challenges have all contributed to low rates of vaccination.

Vaccine doses delivered with short expiration windows have led to only about 63% of the vaccines delivered to the continent being utilized. Furthermore, misinformation has fueled a loss of confidence in science and vaccines resulting in low uptake by the population even in countries where vaccines are available. The emergence of a vaccine tier system has not helped. A significant proportion of vaccines donated through COVAX are vectored vaccines from AstraZeneca and Johnson and Johnson, both of which have been plagued by rare blood clotting adverse effects. These vaccines have essentially been phased out of use in Europe and North America with mRNA vaccines being the preferred option. Many on the continent have viewed with skepticism and suspicion being offered vaccines which albeit effective are no longer used in the high-income countries donating them.

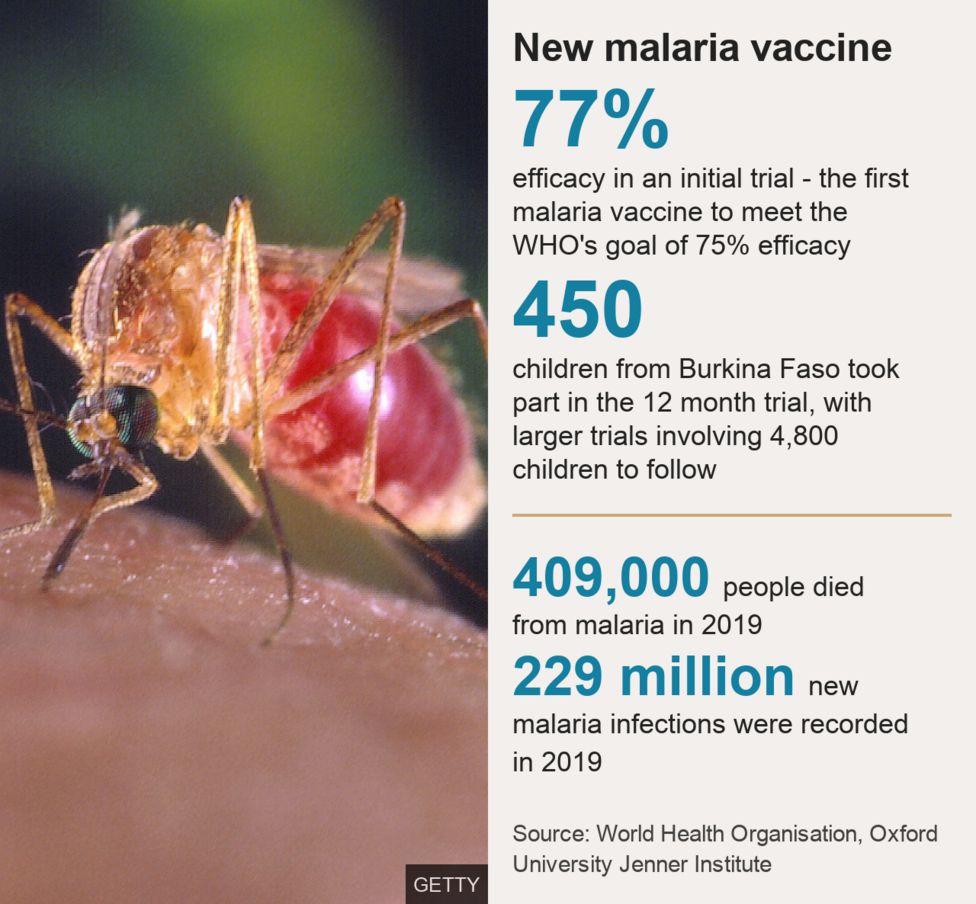
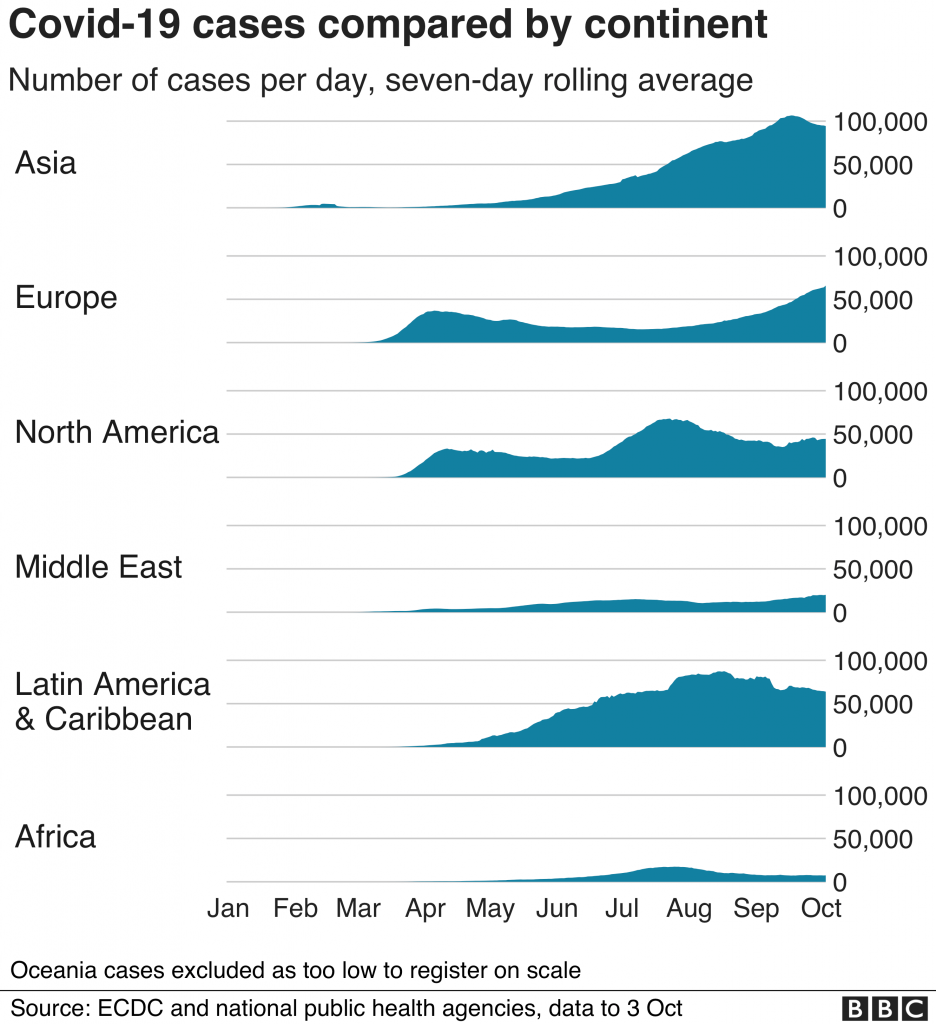
Africa compared to other parts of the world has seen fewer cases and deaths directly from COVID19. Many view the pandemic as of a less pressing health concern than Malaria, HIV/AIDS, Tuberculosis and other poverty related issues. The impact of COVID19 has been devastating for every aspect of healthcare and the economy in Africa. However, it is challenging to articulate secondary benefits of vaccination in public health messaging without addressing immediate pressing concerns.

With new vaccines now authorized and COVAX finally able to increase its supply, it is likely that in 2022 supply will exceed demand and the bigger challenge will be getting the available doses in arms. This will require addressing logistic challenges and barriers to vaccine delivery but also tackling head on the real issues around vaccine hesitancy and acceptability. While the mantra of “vaccinate the world” is attractive, one size will not fit all. A more tailored approach with countries setting realistic targets for their populations is likely to be more acceptable.
The Show Must Go On – AFCON with Omicron surging
Africa has weathered previous waves of SARSCoV2 successfully but the combination of Omicron surging, low vaccination rates and the African Cup of Nations (the continent’s largest sporting event ) brings fresh concerns. For a continent that loves its football, cancelling the competition for a second time was not on the cards. Cameroon will host and many see the success of the Olympics as proof that this can be done safely. However, the conditions in Cameroon leading up to the AFCON are quite different.
:focal(1269x729:1271x727)/origin-imgresizer.eurosport.com/2021/06/06/3147503-64505788-2560-1440.jpg)
Cameroon is among the lowest vaccinated countries in the world. Non-pharmacologic interventions are barely enforced and pandemic is high. The competition will proceed with stadia at full capacity unlike the Olympics where no spectators were allowed. The ministry of health has announced that proof of negative testing and vaccination for entry into stadia. These measures are encouraging but corruption and bribery are rife and it is doubtful how these measures would be enforced. Also vaccine hesitancy is prevalent and testing capacity is low.

As a Cameroonian and a football fan I am rooting for a successful celebration of African football. I hope the resulting surge of COVID19 cases is minimal. The economy of the country needs the boost and the continent needs joy and celebration that accompany the AFCON. However, this hope is tempered with perspective. With omicron we are dealing with the virus in its most infectious variant yet. While the show must go on, the consequences of a massive wave after the games could have significant regional impact.
Despite encouraging signals that omicron may cause less severe disease, a rapid rise in case numbers can be a major stress test for any health system. This has been demonstrated across Europe and North America. The youthfulness of the population in Cameroon (median age 17) and immunity accumulated from previous waves may mitigate the severity of a surge. Only time will tell the impact of the games of the trajectory of the pandemic in Cameroon and Africa. Another situation to watch closely at the start of this new year.

The Virus is Still Speaking – We Should Start Listening
For many the realization has set in that we have to learn to live with the virus. How we choose to do that matters. The start of new year is always an opportunity for a reset and learn from past failures. With COVID19 this means a renewed commitment to global solidarity, not only in words but in action. The approach of every country for itself saw us squander the potential of vaccines and therapeutic advances in 2021. The virus carried on, unperturbed leaving a string of new variants, long-term chronic symptoms and deaths in its wake.

We get a chance in 2022 at a do over, this time with even more tools in the pandemic toolkit. That means living out the words “no one is safe, until everyone is safe” by holding world leaders accountable to end the pandemic. Every moment wasted in repeating old mistakes is another victory for the virus. The virus will keep speaking until we are ready to listen and respond accordingly. That’s our only hope to make this year a better one for us all.
Abbreviations: LMIC – low and middle income countries, HIC -High income country
Written by Boghuma K. Titanji